The Analogy Lab
An inside look at one of NPLB’s fellowship projects, leveraging AI, creative storytelling, and social media.
Let’s tell the story of innovation and the policies that threaten to destroy it.
The Inspiration
The NPLB Biotech Fellowship gives emerging leaders a practical look at how innovation, policy, and patient access fit together. Fellows complete hands-on projects that translate complex issues into clear insights, contributing to NPLB’s broader public-education mission.
For the Analogy Lab initiative, fellows harness analogy-driven storytelling to illuminate the hidden dynamics of our healthcare system.
By turning complicated issues—like insurance design, vaccine trust, global freeriding, or the value of medicines—into visual metaphors, they aim to make hard-to-grasp concepts instantly understandable.

“As a scientist, I focused on how medicines work and on the biology behind potential new treatments. The Fellowship taught me how the system decides who actually gets those medicines. Once I saw that access is determined by insurance design, the whole system came into focus.
“Learning the science made me a researcher; understanding the incentives and the costs pushed onto patients made me an advocate. The Fellowship showed me why cures stall in the real world, driven by misaligned incentives and coverage design.
“The comic series grew out of that realization. A single image can show what policy hides: who pays, who waits, and why the system breaks. I entered science to understand disease; the Fellowship taught me to understand the systems that let disease win.”
— Sofia Brites Boss, NPLB Senior Fellow
Sound exciting? Learn more about our NPLB Biotech Fellowship here.
The Comics
Quickly navigate the comics here:

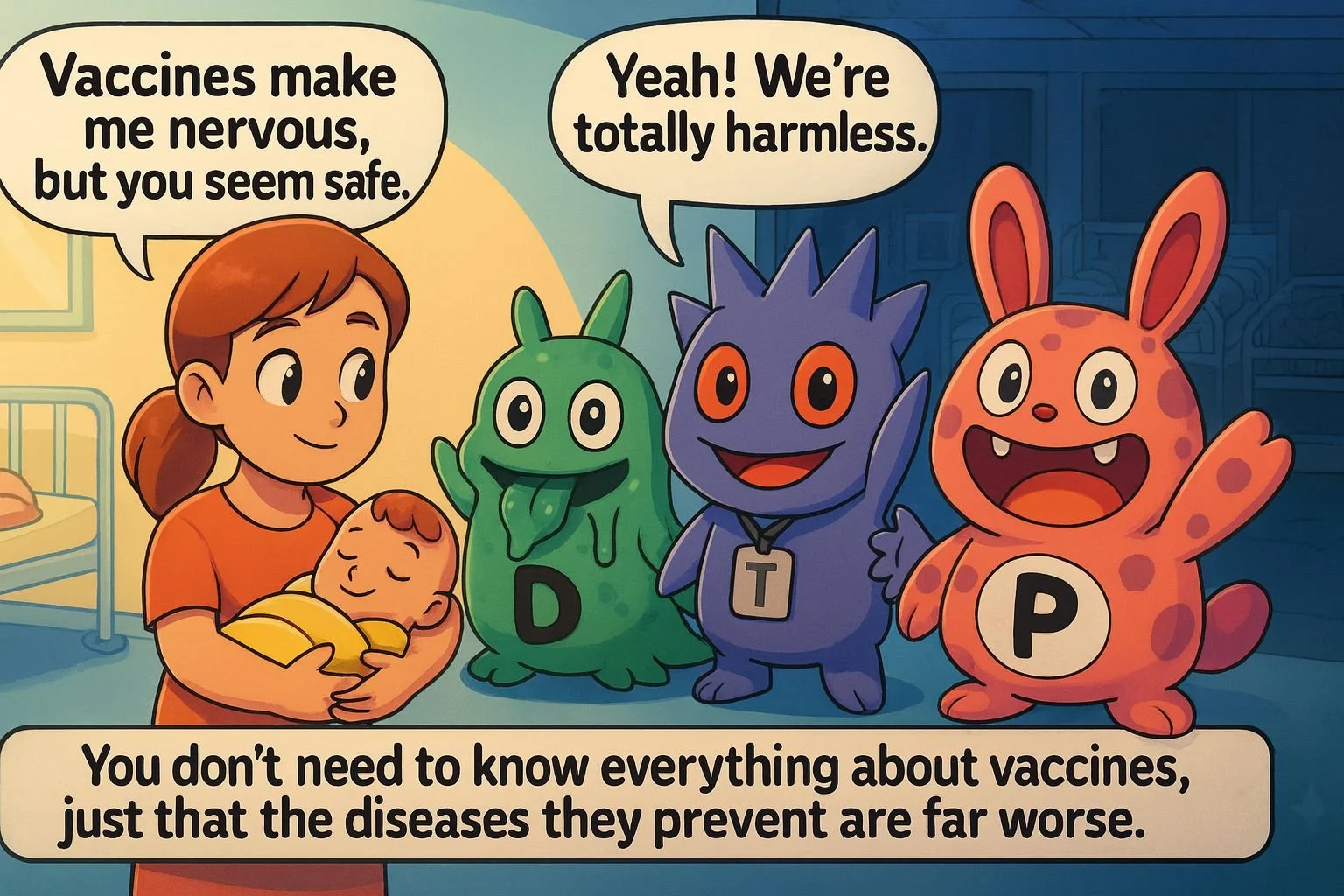




Don’t Trust DTP
No parent misses diphtheria, tetanus, or whooping cough; those infections disappeared from everyday life for a reason. Yet because vaccines pushed them into the background, it’s easy to worry more about the shots than about the pathogens themselves, as if D, T, and P were now “totally harmless.” Before the DTaP vaccine era, the U.S. saw roughly 100,000-200,000 diphtheria cases with 14,000-15,000 deaths each year, 500-600 tetanus cases with about 30 deaths, and around 175,000 pertussis cases with about 9,000 deaths annually; with widespread vaccination, cases and deaths dropped by 95-99%.
You don’t need to know every detail about immunology to weigh that tradeoff: the risks from vaccines are very small and well-characterized, and they’re far outweighed by the protection they give against diseases like diphtheria, tetanus, and pertussis.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)
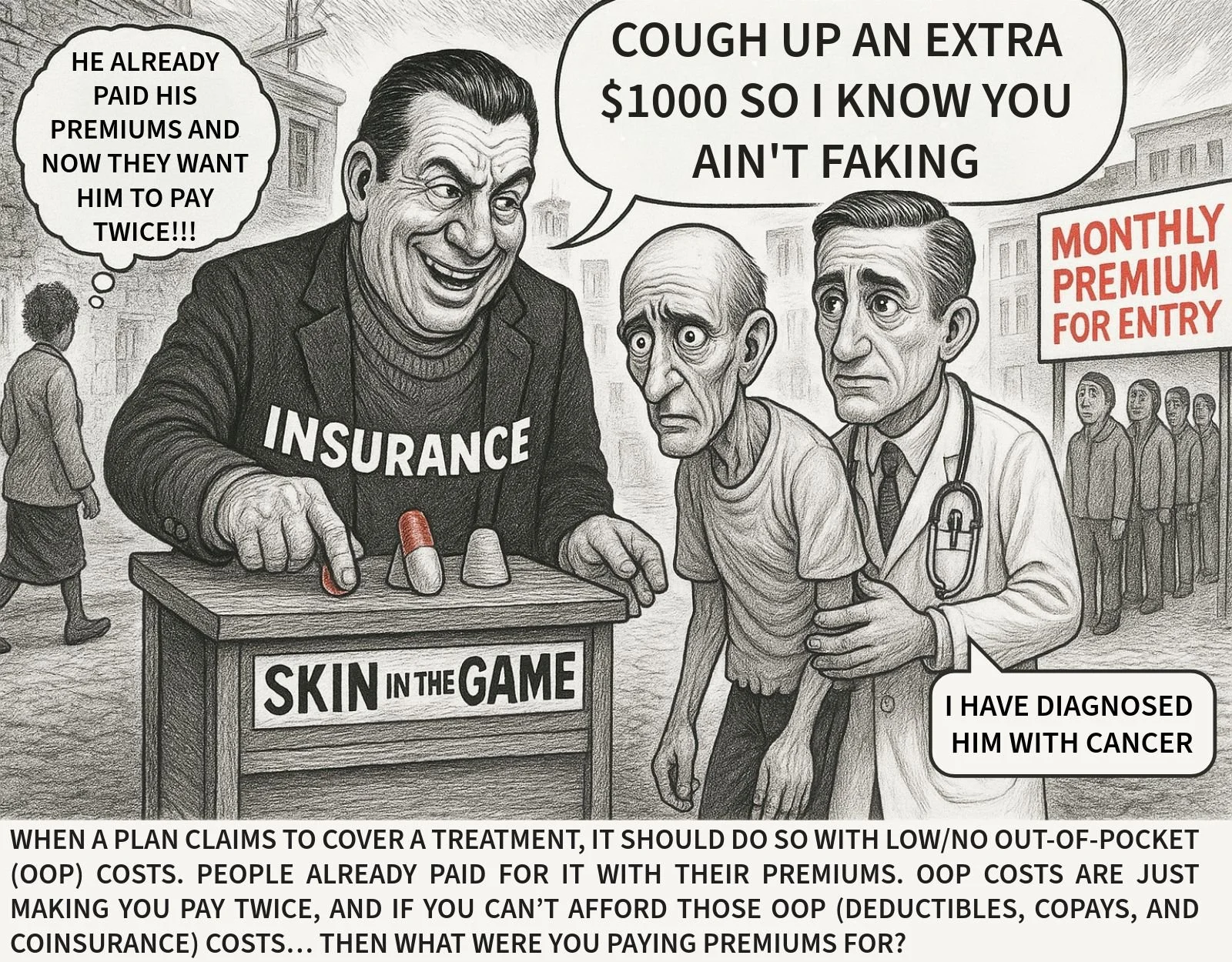
Skin In the Game:
An Insurance Shame
The idea of “financial skin in the game” often just ends up meaning patients pay twice. For cancer, lupus, or diabetes, no one is faking their way to treatment, yet plans still attach on deductibles, copays, and coinsurance on top of years of premiums, so the sickest patients are asked to pay the most. Premiums are supposed to cover the cost when you get sick; if out-of-pocket charges keep people from starting the treatment their doctor prescribes, what were they paying premiums for?
Let’s #FixInsurance so that when a plan says it covers a medicine, patients aren’t billed a second time at the very moment they need it.
Comic by: Darius Walker (NPLB Fellow)
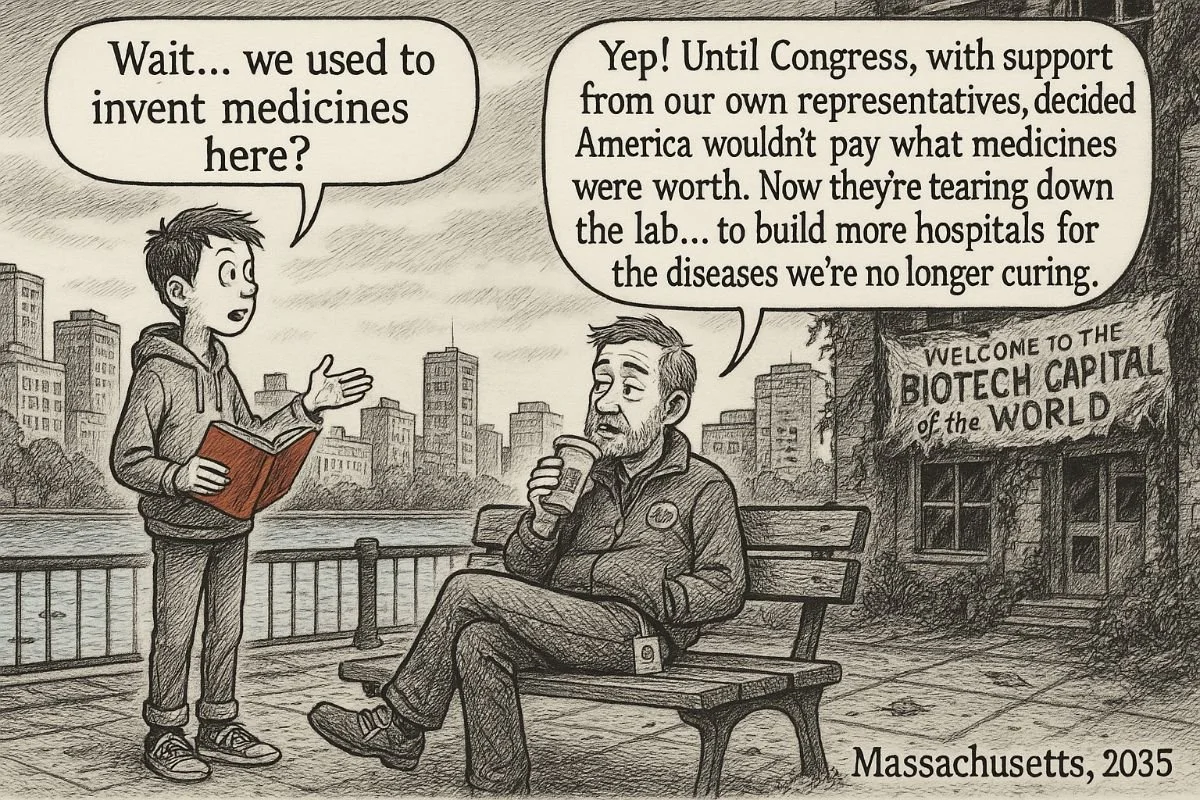
Massachusetts, 2035
Massachusetts is the biotech capital of the world today, but that only holds as long as America is willing to pay for the medicines invented here. If Congress decides that new drugs aren’t worth paying for and leans into price controls instead of fixing insurance, investors will fund R&D somewhere else and the labs along the Charles will empty out while we spend more on hospitals for diseases we could have prevented or cured.
Let’s #FixInsurance so patients can afford the medicines they need without voting away the industry that makes those medicines possible.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)

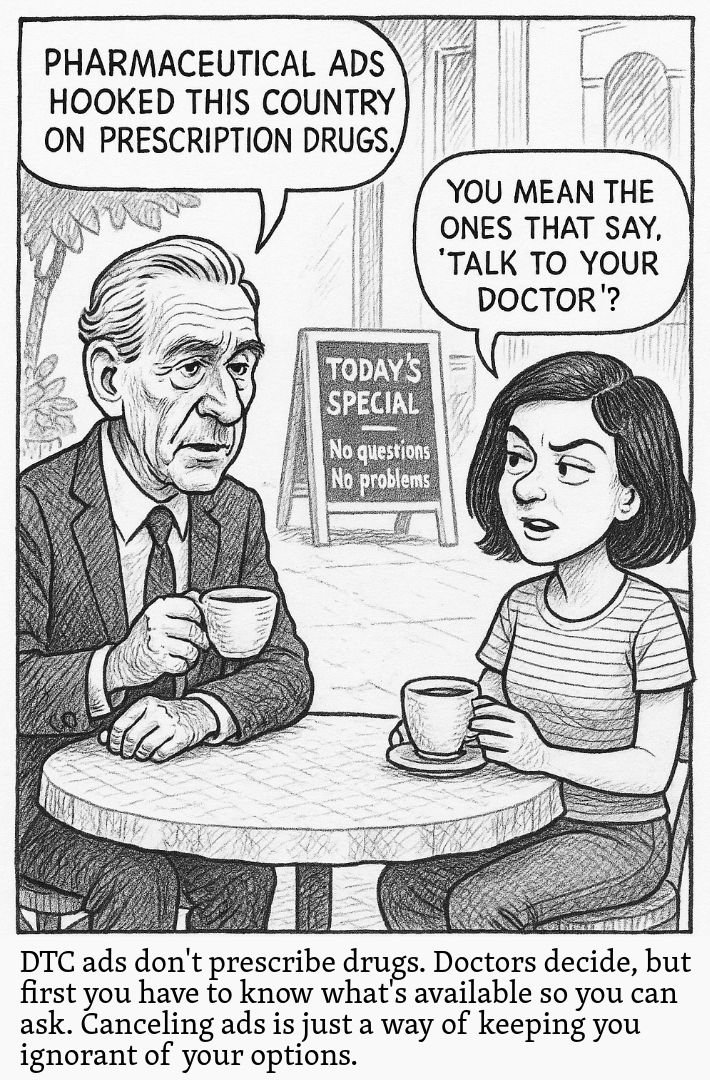
Direct-to-Consumer rug Ads Don’t Prescribe Medicines
A doctor can always say no; what DTC ads really do is let patients know a drug exists so they can bring it up with their physician. If we eliminate that imperfect source of awareness without creating a better on-ramp, the effect isn’t safer prescribing, it’s more patients remaining unaware of options that might help them and less reason to invest in developing and competing on new medicines.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)
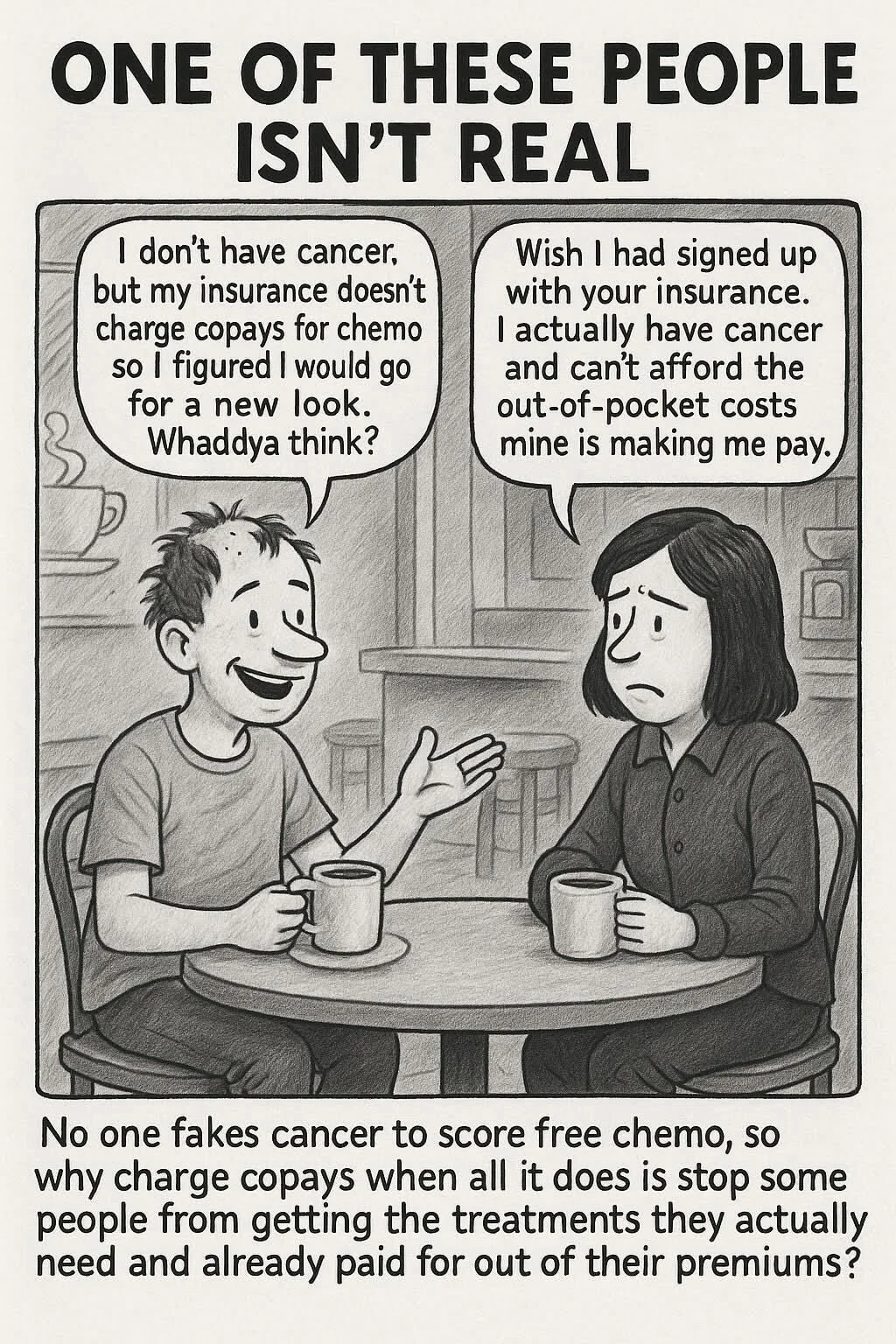
No One Fakes Cancer to Get Free Chemo
People only go through chemotherapy when they and their oncologists think it’s necessary. Yet many health plans still charge deductibles and high copays for chemo on top of years of premiums, as if there were a “free chemo” problem to police. Did you know that once out-of-pocket costs climb above about $2,000, roughly half of patients abandon their prescribed chemotherapy? Why are some health plans designed so that people pay the most when they’re sickest? Let’s #FixInsurance so no one ever has to fight cancer and their health plan just to afford the medicines their doctor prescribes.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)

Measles Isn’t Just a Childhood Rash
It’s one of the most contagious viruses we know, and it can cause pneumonia, brain swelling, and death. Before the measles vaccine was introduced in 1963, the U.S. recorded about 500,000 cases and roughly 400–500 deaths every year, with many more infections and hospitalizations that never made it into the statistics. Vaccination pushed measles out of everyday sight, which makes it easier to worry about “the jab” than about the virus itself. But when the risk from the pathogen is that clear, you don’t need to know every detail about how the vaccine works to see the benefit of giving your child protection instead of giving measles a chance at that hug.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)
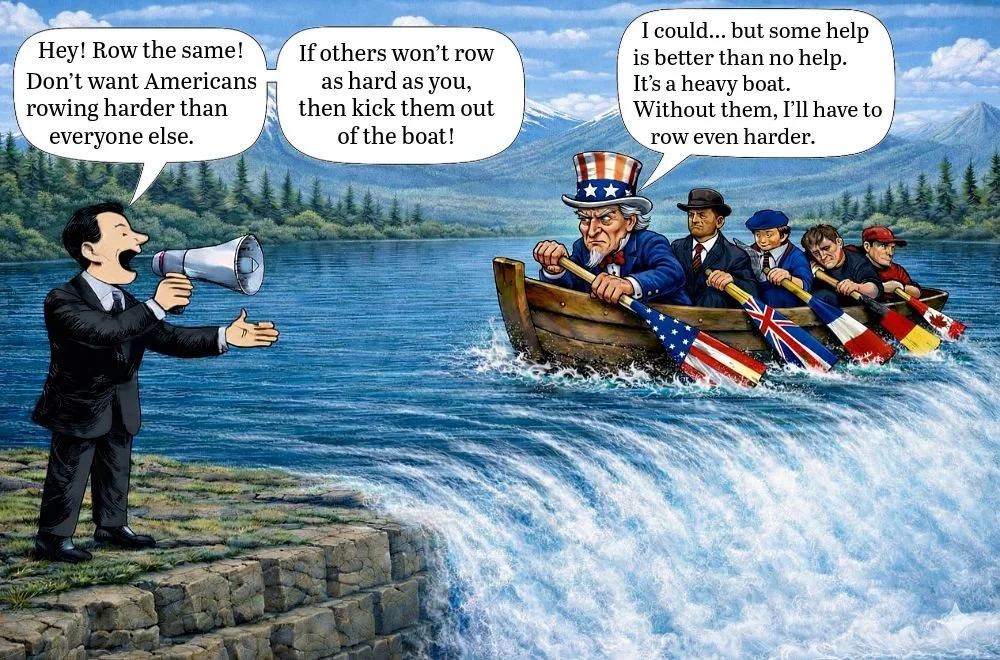
Why MFN Backfires
It’s frustrating to row harder than others, but refusing their help makes no sense when the alternative is going over the disease cliff. The canoe works only if it keeps moving forward, and biomedical innovation depends on sustained investment to do that.
Most Favored Nation pricing forces everyone to row at the same pace; if other wealthy countries won’t row harder, the choice becomes slowing down to match them or tipping the canoe altogether, either way, we lose. We pay more by carrying the burden alone, or we pay later by suffering diseases we could have prevented with new medicines.
Even when drug prices feel high, medicines go generic while disease and hospitals never do, and the roughly 8% of healthcare spending that funds all novel medicines is affordable if spread through premiums rather than concentrated on the sick.
Comic by: Sofia Brites Boss (NPLB Senior Fellow) and Peter Kolchinsky (NPLB Founder)
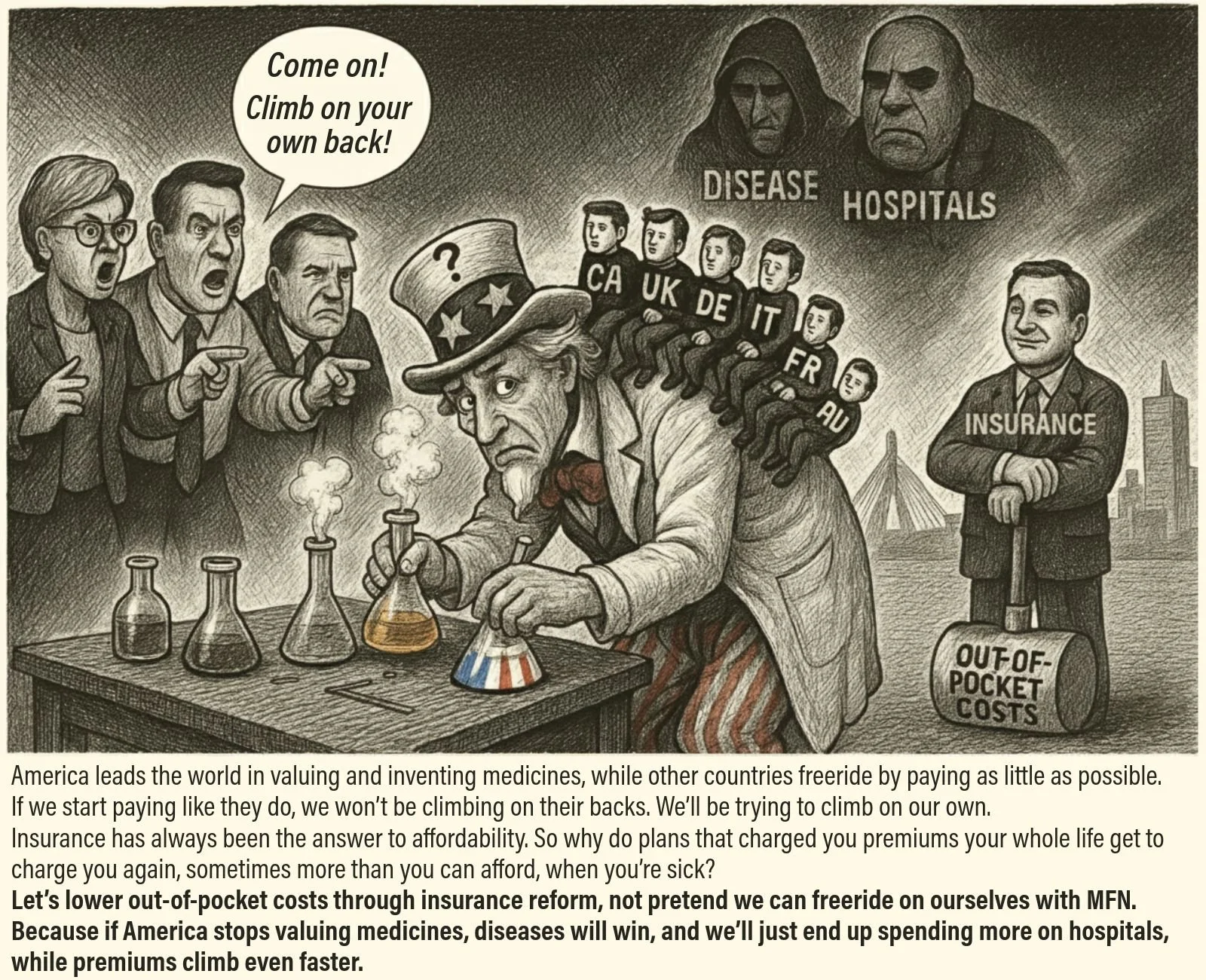
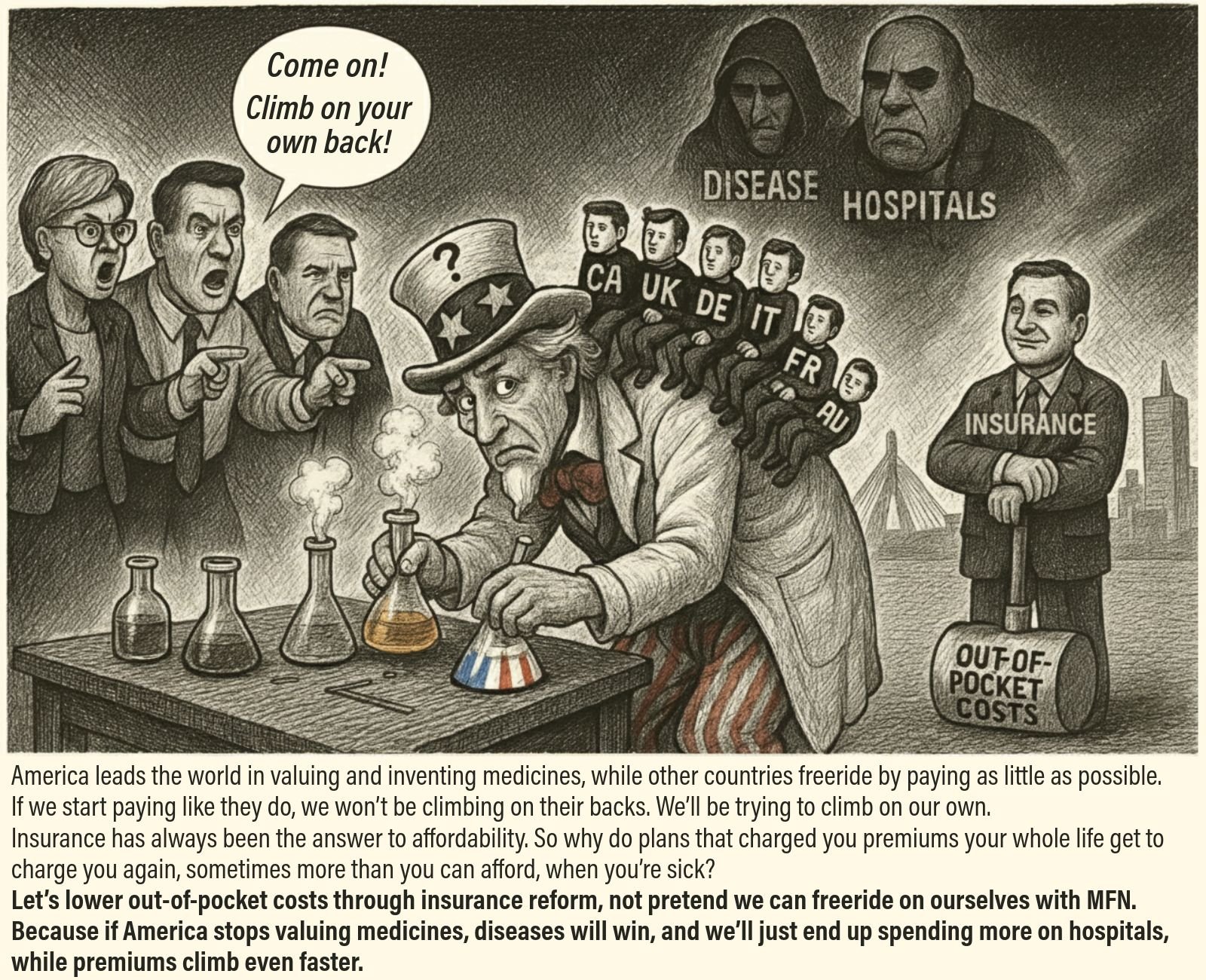
The Global Free Ride
If other wealthy countries pay less for the same medicines, are they really getting a better deal, or just freeriding on America’s investment in innovation? The U.S. supplies roughly half of global drug profits despite being only about a quarter of global GDP, which is why investors are willing to fund so much R&D here while Europe, Canada, Japan, and Australia underpay and rely on those same medicines once they exist. Importing their price controls through policies like Most Favored Nation wouldn’t mean climbing onto their backs; it would mean trying to climb onto our own, shrinking the market that sustains new medicines and shifting more of the spending into hospitals and premiums, when we could instead improve affordability by lowering out-of-pocket costs through insurance reform.
Let’s #FixInsurance, because if America stops valuing medicines, diseases will win.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)
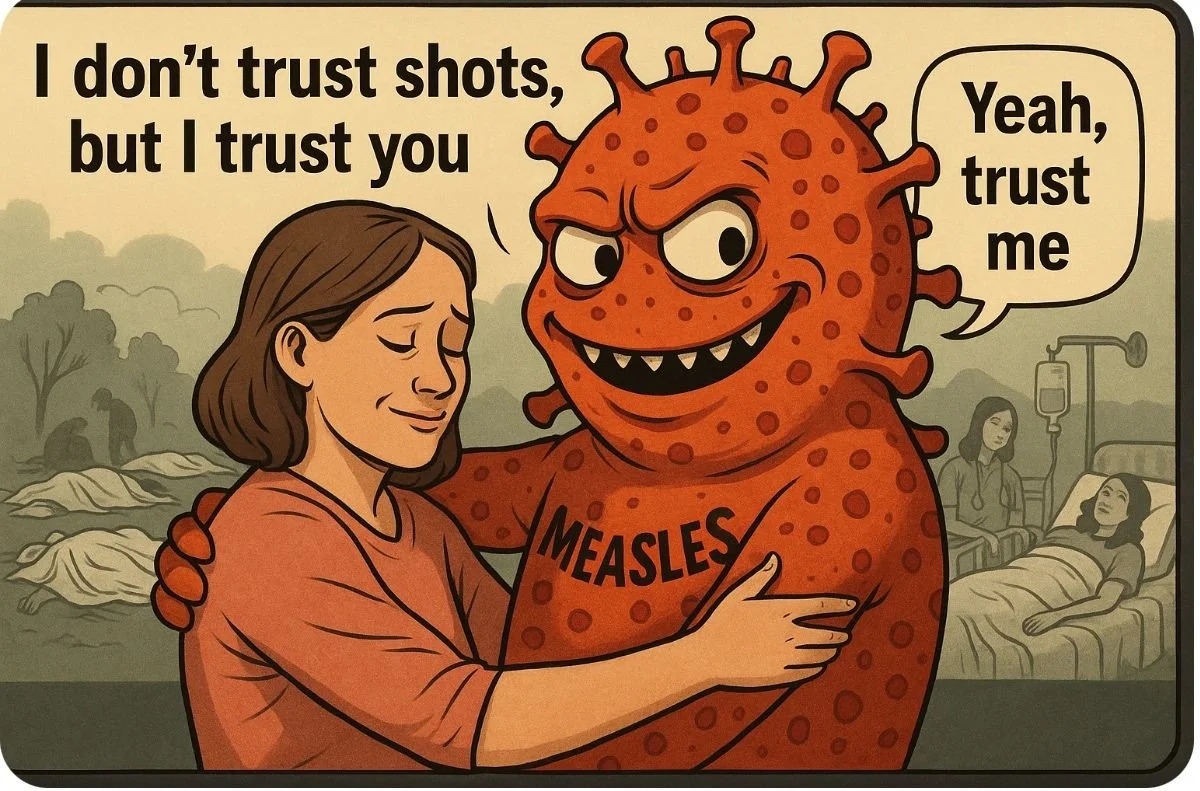
The Measles Monster
Vaccines rely on trust and facts, but sometimes the framing needs to shift. Measles is a deadly disease. It doesn’t need your trust — only your hesitation — to spread. Vaccines rely on trust and facts, but the real threat is the pathogen itself, not the prevention.
You don’t need to know everything about vaccines to support them — you only need to understand even a little about the danger of the pathogen.
Comic by: Peter Kolchinsky (NPLB Founder)

The Massachusetts Paradox
Massachusetts built the world’s biotech capital — more than 1,000 companies, 117,000 jobs, $23 billion in wages, and breakthroughs that cure diseases, save lives, and offer patients hope.
Yet election after election, many patients and voters are being persuaded to turn against the very innovation system that could one day save them or someone they love. Instead of championing policies that protect access, affordability, and continued progress, the Commonwealth keeps empowering leaders whose short-sighted decisions chip away at the engine of medical discovery.
It’s time to protect the ecosystem. Let's make MA fall back in love with a uniquely MA industry that helps make our state amazing and all the world healthier.
Comic by: Peter Kolchinsky (NPLB Founder)
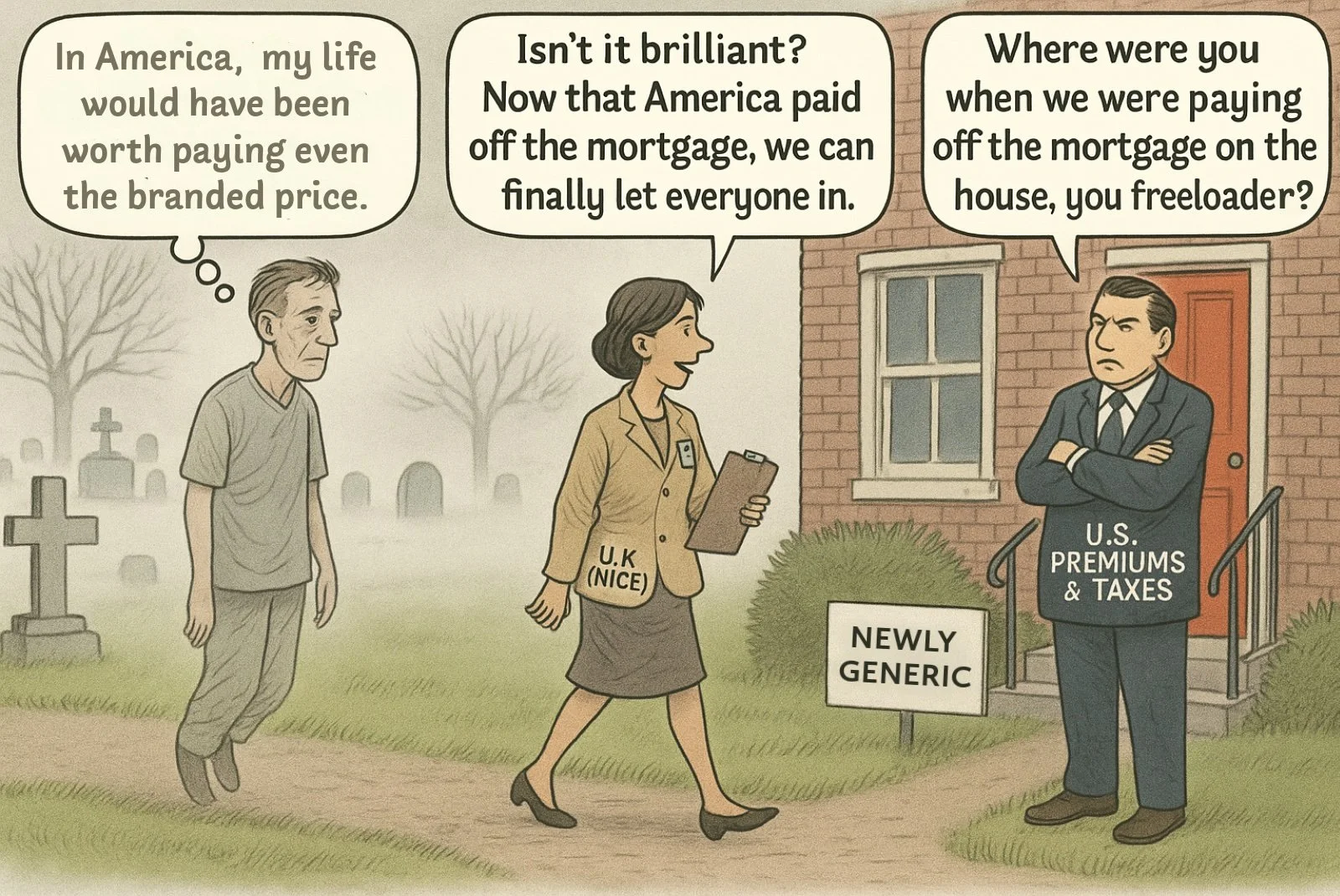
The Mortgage Analogy
Some health systems wait to cover breakthrough medicines because they undervalue them during the branded period and only revisit the decision once generics enter. That leaves the U.S. market to shoulder the risk, fund the R&D, and effectively pay off the mortgage on innovation while others delay adoption.
The cartoon captures that dynamic: a patient who never received treatment because his system waited for someone else to carry the cost. We’ve seen this pattern with CFTR modulators, which several high-income countries delayed despite clear clinical benefit, and with abiraterone, which NICE initially deemed “not cost-effective” until generics made it easier to support. In this case, U.S. payers funded the mortgage. Others moved in once it was paid off.
Comic by: Sofia Brites Boss (NPLB Senior Fellow)
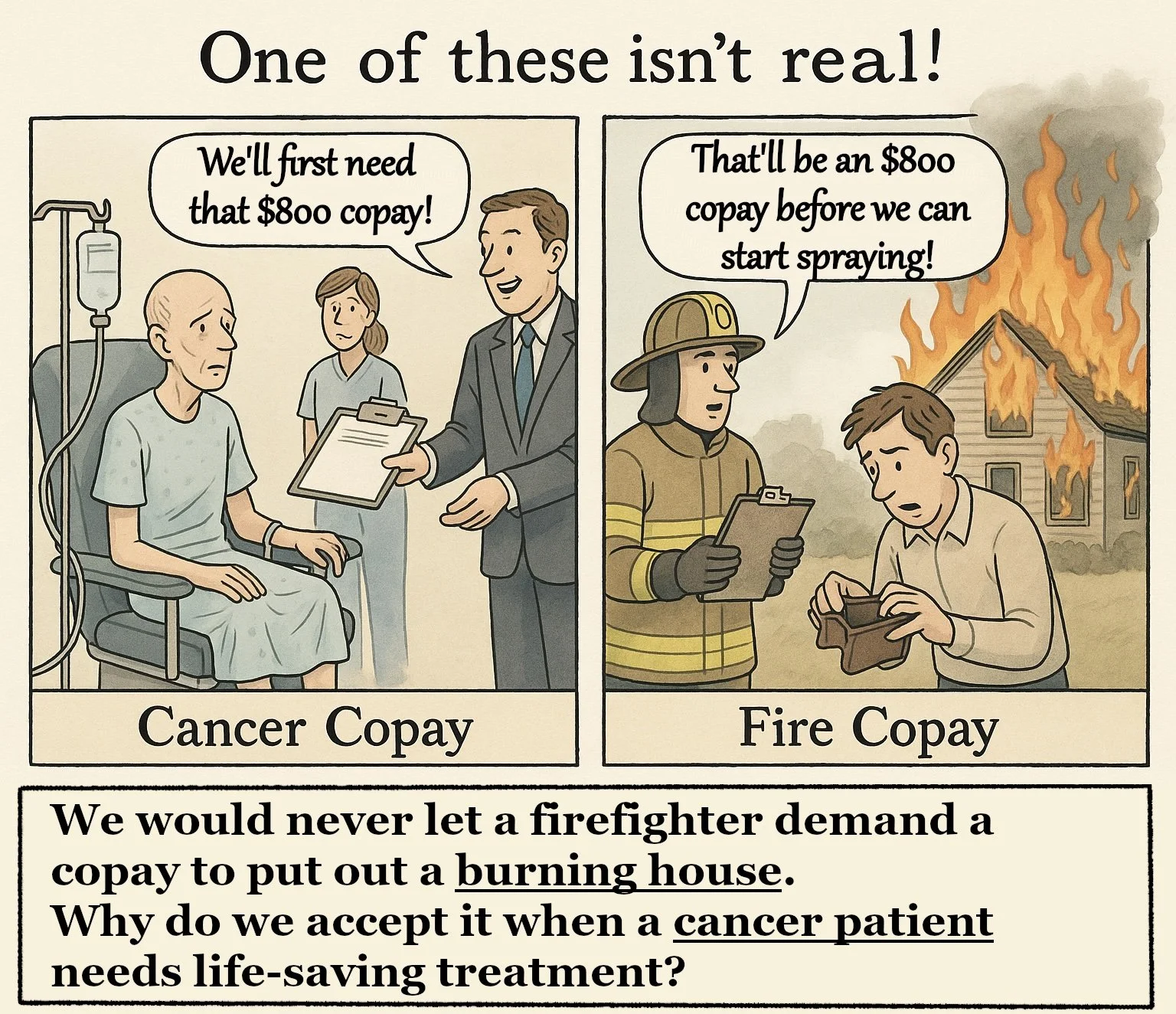
The Firefighter Copay
We would never tolerate a firefighter demanding a copay before putting out a burning house, so why do we accept it for life-saving treatments?
Like the fire department, biopharmaceutical innovations benefit the whole community. This is why we must think of them in the same way as we think of firefighters — we all pay into the biotech ecosystem as a community through our monthly premiums which spread the high cost of risky innovation across all of society. Then, when the moment comes when we need access to a life-saving medication, that drug is free to us. This model matches the firefighter model — with the health subsidizing the sick (and the safe homeowners subsidizing the homeowner facing an emergency), not the other way around.
Comic by: Afshin Seyednejad (NPLB Fellow)
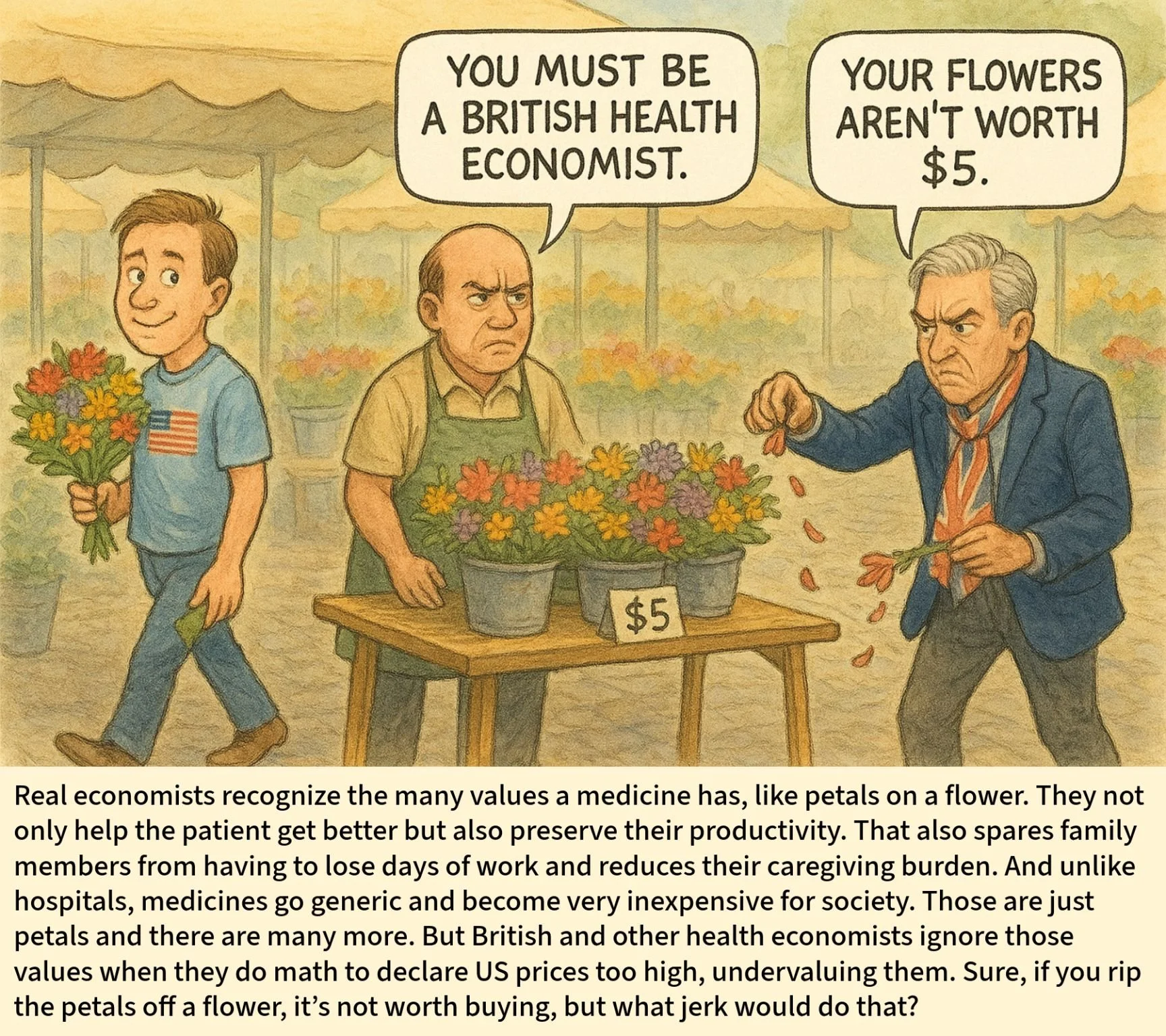
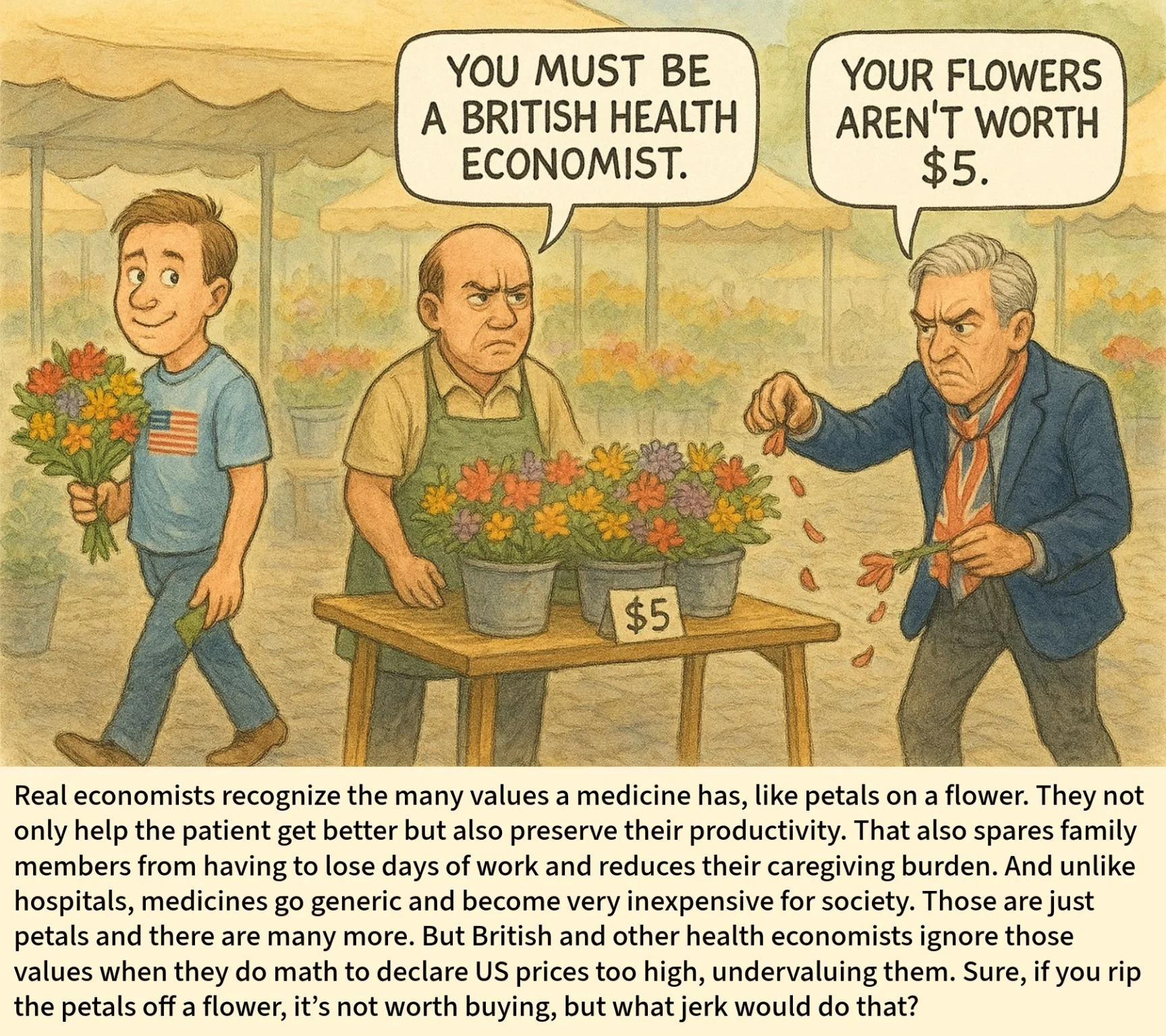
The Value Flower
A medicine’s value is a whole flower, health gains, productivity, caregiver relief, scientific spillovers, and its price naturally falls once it goes generic.
If you pluck those petals off, of course the flower looks “not worth it.” Count them, and coverage with low out-of-pocket costs suddenly makes sense.
Comic by: Clara Brouaux (NPLB Fellow)

Tiny Cost, Vast Reward
The 1.4% of the US GDP spent on new medicines each year not only funds today’s healthcare but also drives future progress.
Price controls like the pill penalty and Most Favoured Nation risk stifling that innovation.
Comic by: Jaime Arroyo de Lagasca Encinas (NPLB Fellow)
We’re building support across the biotech ecosystem
BECOME A FIRST RESPONDER & THOUGHT PARTNER
Sign up to receive action alerts. Help protect access to lifesaving medicines & preserve innovation for those still waiting for a cure.
JOIN THE NPLB BIOTECH FELLOWSHIP
Participate in live lessons, connect with like-minded fellows plus industry leaders in biotech, and collaborate on impactful projects.